Abstract
Over the past decades substantial progress has been made in addressing health disparities of people with intellectual disability. The “era of awareness” (pre-2005) identified a “cascade of disparities” of more adverse health conditions, less attention to health needs, poorer health care access, and fewer opportunities for health improvement. This occurred alongside emerging governmental recognition of the poor health of people with intellectual disability. The “era of assessment” (2005-2015) saw advances in improved health data, population health surveillance, attention to environmental contributors, and passage of the Convention on the Rights of Persons with Disabilities. Research extended from clinical samples to population-based studies with greater focus on social determinants of health. The “era of context” (2015-2025) was characterized by the COVID-19 pandemic, technology, and greater inclusion of people with intellectual disabilities in their communities. Data advances included a disability data framework, clearer disability definitions and identification, and greatly expanded data-linkage research to inform programs and policies. Disability health competencies were developed in multiple countries for multiple disciplines. For the coming decade, we anticipate greater use of technology, especially Artificial Intelligence, expansion of the “inclusion movement,” and attention to ableism. Data linkage and analysis in multiple countries will map longitudinal health trajectories. We anticipate a much-needed resurgence in attention to mental health. Global climate change will demand inclusive emergency preparedness. Future advances require that research, health care, service programs, and communications be co-designed with people with intellectual disability and their supporters. Focus and funding are critical through investment proportionate to need.
Introduction
Poor health among people with intellectual disability has been recognized for decades, with a substantial but undetermined portion considered preventable disparities (1–6). Although the persistent reports of health disparities might suggest little advance, the authors believe significant progress has been made in identifying, measuring and improving the health of people with intellectual disability. Meaningful changes, both minor and major, typically occur step by step, with advancement building on previous progress both within the health domain, and in conjunction with broader, cross-sector transformations. This paper reviews advances over the past thirty years, summarises our perspectives based on a broad review of the literature and our knowledge of developments, highlights areas requiring more rapid progress, and suggests future directions to advance health care for people with intellectual disability. The authors write from positions as academic researchers in the U.S. and Australia. The first author has experience in U.S. federal government service and public health programs and policies; the second has engagement with Australian health services, regulatory bodies and policy. The paper is limited to English-language publications and primarily high-income countries.
Step-by-step progress in the recent past
Era of awareness (to 2005)
National reports
From 2001 to 2005, a number of countries including the UK (7), USA (8), Scotland (9), Australia (10), and Canada (11) issued national reports highlighting poor health among people with intellectual disability. These reports focused on early detection, reducing comorbidities, and empowering individuals and carers to improve health outcomes (12). In 2001, the World Health Organization published the International Classification of Functioning, Disability and Health (13) which for the first time, identified environmental factors alongside personal factors and health condition as influencing health and function. This further promoted incorporation of the social model of disability into understanding health.
A cascade of disparities
A 2006 review (12) identified that much of the previous literature related to unique health needs of clinical samples, finding under-diagnosis of health conditions (14, 15), over-prescription of anti-psychotic drugs, and diagnostic overshadowing (15, 16). People with intellectual disability experienced “a cascade of disparities,” with each disparity compounding the effects of others. First, they experienced more adverse health conditions including epilepsy, heart conditions, mental illness, poor oral health, vision and hearing problems (2, 16–20). While some of these problems related to the disability etiology (e.g., Down syndrome), others were preventable. Second, they experienced disparities in attention to their health care needs, due to communication differences, behavioral concerns, inconsistency in supports, and delays in seeking health care (15, 21–24). Third, the literature documented disparities in access to quality health care related to clinicians’ lack of training and expertise, and difficulties with logistics like transportation (23–25). Finally, people with intellectual disability experienced disparities in preventive care and health promotion, with fewer opportunities to learn how to improve health behaviors and adopt healthier lifestyles (15, 16, 26, 27). This cascade of disparities led to poor health outcomes.
Self-determination
This period also witnessed growth in the self-determination and person-centered planning movements that had been initiated in the 1980’s. Advocacy groups implemented curricula to teach self-determination skills to adolescents and adults with intellectual and developmental disabilities, and self-directed supports became a guiding principle for service delivery (28). Clinical and community researchers developed and tested a number of health intervention tools. Examples included the ASK toolkit to promote self-advocacy for better health care (29), the CHAP checklist for general practitioners to attend to all relevant areas of health (30), and evidence-based curricula on health and healthy lifestyles for people with intellectual disability (31, 32). While this period was characterized by greater attention within the disability community to preventable poor health, the need persisted in broader policy and service systems for increased awareness and improvement.
Era of assessment (2005-2015)
The next decade marked dramatic improvements in assessing the health disparities of populations with intellectual disability. Data-driven decision-making for the general population demanded the same approach for people with intellectual disability, resulting in calls for action to address disparities (33, 34). Attention shifted from conditions unique to people with disabilities to comparing their health with the general population using health indicators. The POMONA project (35–37) showed that health of people with intellectual disability could be assessed using 18 common health indicators across 13 European countries, filling a critical measurement gap and revealing a consistent burden of preventable conditions, lifestyle risk, and care‐quality shortfalls across Europe.
Role of environment
Environmental factors identified in the ICF framework gained much more attention, especially Social Determinants of Health (SDOH) SDOH frameworks were published by WHO (2008) (38), the European Commission (2009) (39), UK (2010) (40), Australia (2010) (41), USA (2011) (42), Canada (2015) (43) and Taiwan (2016) (44). Some frameworks focused on “causes of causes” such as macro-economics, early child development, and social policies (45), while others were more individual-focused covering economic stability, education, health promotion and health care, neighborhood and built environment, and social and community context.
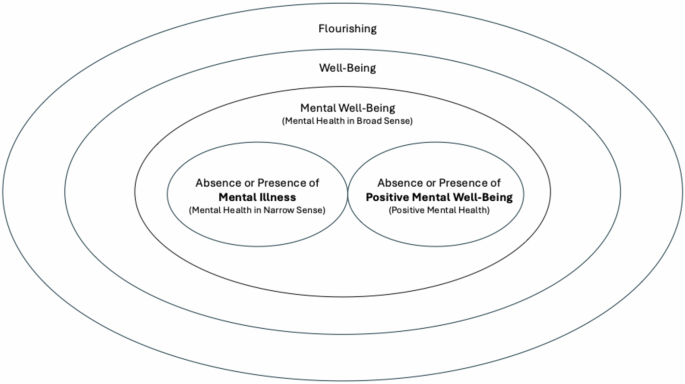
Changes in foci of interest
As indicated in Figure 1, over time, health indicators broadened from morbidity and mortality to include quality of life measures (e.g., self-reported well-being, self-determination, life satisfaction), health behaviors (e.g., smoking, nutrition, and physical activity), environmental factors, and subsequently, mental health (46–48).
Improved health surveillance
This decade experienced major improvements in disability health data and surveillance and a shift from clinical samples to population level surveillance. The United Kingdom’s Learning Disabilities Observatory (~2010-2020) published key population studies (49) and identified the “transition cliff”, a precipitous drop in prevalence in administrative data between childhood and adolescence to early adulthood (50). Use of health services research with administrative datasets revealed disparities such as more hospitalization for ambulatory care conditions like diabetes for people with intellectual disability (51).
Linked data
Between 2005–2015, the use of large, linked datasets and advanced “big data” capabilities emerged in several countries. Routine digitization of clinical and administrative data and strengthened stewardship enabled integrated linkages and analyses of factors affecting health outcomes. In Canada, Manitoba’s unique integrated data repository allowed investigation for people with developmental disabilities (34, 52), while in Australia, Leonard’s research group used intellectual disability registry data with other data sets to study the health of people with intellectual disability identified from birth onwards (53, 54). Governance advanced through privacy‐preserving linkage, controlled output disclosure, and audit trails. Despite progress, challenges with data completeness, coding fidelity and sample bias remained, underscoring the need for careful interpretation.
Chronic conditions
Marking a shift from conditions unique to people with disabilities, chronic conditions emerged as major contributors to poor health of people with cognitive disabilities. People with physical, cognitive or intellectual disabilities were documented to be at much higher risk for a number of chronic conditions, including diabetes and cardiovascular disease, and to experience them at earlier ages than the general population (55–58). Recognition of multimorbidity as a major contributor helped refocus the understanding of poor health of people with intellectual disability.
Era of context (2015-2025)
COVID-19
The COVID-19 pandemic was the major health event of the decade, disproportionately affecting people with intellectual disability due to higher susceptibility to infection and death (59–61). This likely related to group living, personal care from itinerant providers, and higher rates of pre-existing health conditions. People with intellectual disability likely also experience more long COVID, though research is limited (62). The pandemic spurred calls for improved health data (63), telehealth and online supports (64), and remote work and socializing–changes that benefited some but also led to isolation and anxiety (65).
International reports
During this decade, the United Nations released the Flagship Report on Disability and the SDGs (66, 67) that, for the first time, included disability in the economic goals for development. WHO developed the Global Report on Health Equity for Persons with Disabilities (68) that brought attention to systemic contributors to health inequity, documented evidence across countries, and made recommendations for country-level actions with an initiative in 2025 to implement recommendations (69).
Improved health data and surveillance
Over the past decade, health data capabilities progressively matured in some countries. Notably, secure analytic platforms provided controlled access to linked unit-record data. Research adopted robust causal methods and transparent reporting. In Australia, this progress was underpinned by Australia’s National Digital Health Strategy 2023–2028. The Australian disability data framework (70), developed with input from people with lived experience, clearly defined necessary health data, current availability, and further data needs, serving as an international model. Aitken and colleagues (71) reported on various methodologies for constructing disability identifiers to link administrative datasets. Investments in large, linked data assets have improved researcher access, with national exemplars being England’s National Health Service (NHS) Learning Disability Data Hub (72), and Australia’s National Disability Data Asset (NDDA) (73) and National Health Data Hub (NHDH) (74). In Canada, where health care and other services data are provincially managed, a national (75) and some provincial datahubs (76–78) enable secure environments with access for researchers. In contrast, the USA lacked extensive health data linkages. Instead, the focus was on standardizing operational definitions for intellectual and developmental disabilities in administrative data to improve interpretability and use (79) (80, 81), ultimately supporting emerging efforts at data-linking.
Population-scale data linkages led by the second author’s team, enabled Australian studies on health service use, costs, comorbidities, and key health outcomes for people with intellectual disability (82–85). Analyses revealed significant gaps in life expectancy (86) and higher rates of potentially avoidable mortality (87). These findings informed interventions and shaped Australian policy to address health inequities.
National roadmaps to enhance health data for individuals with intellectual disability include routine identification in electronic health records and expanded data capabilities and comprehensive outcomes reporting in Australia (88). In the USA, data improvements call for the identifiers in national health surveys, standardizing analytic methods, increasing state research and analytic capacity, and improving communication about prevalence, health needs and health (89).
Mental health
Previous work in intellectual disability mental health identified the need for training (90–92), and this decade brought substantial advances in documenting and responding to the high mental health needs of this population (93, 94). Population level data linkages demonstrated elevated rates of mental illness (95), ineffectiveness of mainstream services (84, 96), and heightened vulnerability during key life transitions, including markedly increased dementia risk (95). Investment in targeted mental health initiatives remained limited, however, with few large-scale programs to build mainstream service capability or expand specialist care. Exceptions were the non-profit National Association for Dual Diagnoses in the USA (91), emerging programs in Queensland (97), New South Wales (98) and Victoria (99) in Australia; and sustained commitments in the NHS in England (100). Mental health services remain a gaping need for persons with intellectual disability.
Technology
The internet and social media greatly expanded opportunities for people with disabilities. Mobile apps enhanced accessibility for people with intellectual disability or limited literacy. For example, apps simplified text, simplified platforms, and supported information access and research participation for people with intellectual disability (101, 102). Advances in artificial intelligence (AI) began to reshape accessible information production for people with intellectual disability by coupling automated language simplification, inclusive design work-flows and assistive reading technologies. AI-enabled Easy Read authoring platforms enabled rule-guided simplification with context appropriate imagery across print, web and audio formats such as Photosymbols’ EasyMaker (103), while symbol-based environments streamlined creation of social stories, and visual timetables such as Widgit Online (104). Reader aids provided rapidly adjustable text, read-aloud and translation features without replacing Easy Read design (105, 106). These rapid developments await rigorous testing and require oversight and monitoring for mitigation of bias in sensitive domains.
Anticipated directions for the future to 2035
Era of inclusion
We are optimistic that dramatic progress in health of people with intellectual disability can be achieved over the next decade. Advances require focus and funding; both have been critical in the past to build infrastructure and fund research and programs. Keys to immediate progress include addressing ableism in health care and public health; longitudinal research; emphasizing integrated, person-centered approaches; supporting data-enabled health ecosystems with inclusive governance; harnessing technology, including AI; improving workforce capabilities; and inclusive planning and management for disasters (see Table 1).
| Anticipated direction | Recommendations for full and equitable impact |
|---|---|
| Inclusion and Ableism | • Include people with intellectual disability and their carers in planning, implementation and monitoring of all health services and programs affecting them • Develop tools and incentivize their use by health care professionals, service providers, and researchers to self-examine and self-monitor for ableism • Mandate ableism training for professionals and service providers, developing additional resources as needed |
| Workforce capability and systems change | • Train across disciplines for health competence in serving people with intellectual disability • Ensure leadership roles in workforce development and educational initiatives for people with intellectual disability |
| Integrated, people-centered care and services | • Examine health systems for discriminatory practices, develop improvement plans, and monitor implementation and effectiveness • Develop and rigorously evaluate approaches and technologies that improve cross sector and stakeholder collaboration in health care |
| Data-enabled ecosystems with safe, inclusive governance | • Ensure interoperable disability flags in all mainstream health and human service systems to improve visibility of population health outcomes • Develop accessible, interactive health outcomes dashboards for use by people with disability, services and policy makers; ensure minimum delays in data feeds • Develop methodologies to support enhanced inclusion of people with intellectual disability in population health data research and monitoring |
| Technology and artificial intelligence | • Determine the priorities and perceived utility of technology and AI from the viewpoint of people with intellectual disability and their supporters • Include people with intellectual disability in planning and implementing new technologies |
| Resilience to climate-related emergencies and other disasters | • Assess the specific vulnerability of people with disabilities to climate change and conduct co-designed research to inform mitigation strategies • Include people with intellectual disability and carers in preparedness planning, disaster management, and post-event monitoring and recovery |
Anticipated directions and recommendations for the future decade to improve health of people with intellectual disability.
The power of together—inclusion and ableism
The intent of the UNCRPD (107) is increasingly being realized in many countries, though less so in the USA which has not ratified CRPD. We anticipate inclusive approaches in research (108–110), disaster planning (94), and communication will become more routine and refined. However, inclusion is revealing rampant ableism, including among health care professionals, service providers and researchers. Research documenting ableism (111–113) is calling us to consciously alter our assumptions and behaviors. Much like sexism and racism, reducing ableism will take time but be transformative for the health and wellbeing of people with intellectual disability. To address previous lack of exposure in curricula, we advocate for routine bias training for all health staff, grounded in lived experience.
Lifecourse approach and longitudinal studies
A lifecourse approach seeks to understand the health trajectories of persons with ID by identifying life-tasks and critical events at different ages and identifying relationships among outcomes over time. Swanson’s conceptual model developed for children with spina bifida (114) has been extended to older populations with intellectual disabilities (115). Two longitudinal studies, IDS-TILDA study in Ireland and HA-ID in the Netherlands have followed cohorts of aged individuals with ID over multiple timepoints, documenting longitudinal changes in health, social circumstances, and mortality (55, 56, 116, 117). Alternatively, linking administrative data sets is providing another view into longitudinal changes (118, 119). We anticipate greater use of lifespan approaches and longitudinal designs in the future.
Health workforce capability, practice standards and health system change
To effect improvements, the future health workforce must possess the confidence, skills, and experience to deliver tailored health care and public health programs for people with intellectual disability. Following a specialty model, the Netherlands initiated a 3-year specialty training of ID physicians in 2000 and subsequent guidelines for adolescent transition of care (120), and the UK and Ireland developed ID nurse specialists (121, 122). Following an inclusion model, some jurisdictions such as the U.K. mandate intellectual disability training for the health and social service workforce (100), while in others, professional development depends on individuals proactively seeking out opportunities. Australia and Canada provide comprehensive capability development resources for health professionals (123–125), while in the USA professionals have developed competencies for health (126) and public health professionals (125). To ensure meaningful impact, intellectual disability content should be mandated in all health professional continuing education curricula.
However, disability‐competent practitioners cannot improve outcomes without supportive health systems. Systemic barriers persist, including discrimination in accepting patients, inadequate appointment lengths, poorly adapted communication or intervention programs, challenges in finding and referring to specialty services, and policies that directly or indirectly limit access to medical equipment, vaccines, treatments, and organ transplants. As systems face greater accountability for population outcomes, they must identify and address systemic barriers.
Strengthening integrated, people-centered care and services for people with intellectual disability
The WHO’s Fourteenth General Programme of Work (GPW14) frames a threefold mission—promote, provide, protect—that links social determinants, strong primary health care, and system resilience (127). This vision will only be realized if accountability measures for equity and key performance indicators important to people with intellectual disability are included in public health and primary and preventive care. People with intellectual disability need to be factored into all broader health systems transformations. For people with intellectual disability, responsive systems require supportive decision-making, accessible communication, continuity of care across transitions, and reasonable adjustments embedded in hospital and health care policies and standards. Routine use of patient reported outcome and experience measures is pivotal to understanding what matters to people with intellectual disability. National health care regulatory standards need actionable measures that raise health care quality, reduce harm, and improve outcomes. Aligning service models with WHO’s integrated, people-centered services will promote care that is co-produced, culturally safe, and coordinated across the life course (127).
Data-enabled ecosystems with safe, inclusive governance
Delivering and monitoring equitable improvements for people with intellectual disability requires cross-sectional and longitudinal analytics with adequate privacy protection and accessible reporting. Jurisdictions will need to prioritize linkage between disability, education, social services, health services, and mortality datasets. Data fields need to include SDOH, hospitalization, primary care (including health checks), medicines, immunization, cancer screening, chronic conditions and cause of death, to ensure adequate capture of outcomes. Routine cohort and subgroup reporting, including all major diversity characteristics, is important to understand the distinct needs of this heterogeneous population. As single source ascertainment of disability status within administrative data is inadequate (128), a key challenge is uniform adoption of disability-specific indicators across administrative datasets. Indigenous data sovereignty principles must guide all analyses and public reporting in Australia (129, 130); in the USA and elsewhere, data analyses should disaggregate by race, ethnicity and other marginalized identities (131).
Technology and artificial intelligence
Advances in AI can expand access to health information for people with intellectual disability by transforming both content and delivery of communication. Carefully governed generative language models with visual supports and multilingual options can automatically produce Easy Read versions of health materials at point of need such as procedure preparation, appointment letters, care plans, emergency preparation information. Inclusive chatbots will provide accessible, cited health information using speech/AAC and iconography, with safeguards that escalate to human support as needed. While accessible explanations can be generated automatically, clinician review will remain essential for accuracy and inclusive decision making.
To realize full impact, these future systems must be co-designed with people with intellectual disability and their supporters to ensure readability, acceptability, truthfulness, actionability, and scalability. Access to technology will need to be ensured for low-income groups to reduce the technology-access gap and realize equitable improvements. Finally, future health navigator models are needed that combine human support with AI-enabled digital coordination (appointments, reminders, transport, benefits, cross-sector referrals) to reduce fragmentation across general practice, specialist care, allied health, and disability services.
Resilience to climate-related emergencies and other disasters
As part of the global population, people with intellectual disability will face more frequent disruptions, with substantial impacts on safety, health and wellbeing (132). WHO’s GPW14 embeds climate risk and emergency preparedness into system planning (127), and jurisdictions must prepare for those most vulnerable. This requires inclusive preparedness planning (e.g., evacuation or sheltering in place), support during events (e.g., access to needed equipment, vaccines, or medications), and post-event recovery supports (133). Equity-sensitive emergency planning must include people with intellectual and other disabilities, and provide accessible alerts, backup virtual care, secure medication and equipment supply chains, and proactive welfare checks. Co-design and strong cross-agency linkages, for example between disability and health services, should be standard in emergency preparedness.
Conclusion
Although health disparities continue for persons with intellectual disability, significant progress has been made in awareness of the need, improved methods for measuring and understanding the reasons for preventable poor health, and recognition of the impact of environmental contributors to poor health. Attention to ableism, longitudinal research, improved capability of health work forces, integrated services, expanded use of data linkage, technology, and inclusive disaster planning are anticipated to be key directions for the coming decade. Focus, funding and inclusion of people with intellectual disability and their families is essential for real progress in the future.
Statements
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
GK: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. JT: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declared that financial support was received for this work and/or its publication. JNT received funding which contributed to this work from the Australian Government Department of Health, Disability and Ageing, and from the National Health and Medical Research Council (Investigator Grant, GNT2009771).
Conflict of interest
The author(s) declared that this work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor HML declared a shared consortium with the author JT at the time of review.
Generative AI statement
The author(s) declared that generative AI was not used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
-
MitraMLong-BellilLMouraIMilesAKayeHS.
Advancing health equity and reducing health disparities for people with disabilities in the United States: Study examines health equity and health disparities for people with disabilities in the United States. Health Affairs. (2022) 41:1379–86. doi: 10.1377/hlthaff.2022.00499. PMID: -
BeangeHMcElduffABakerW.
Medical disorders of adults with mental retardation: A population study. Am J Ment Retard. (1995) 99:595–604.
-
EmersonE.
Health status and health risks of the “Hidden Majority” of adults with intellectual disability. Intell Dev Disabil. (2011) 49:155–65. doi: 10.1352/1934-9556-49.3.155. PMID: -
EmersonE.
Inequalities and inequities in the health of people with intellectual disabilities. In: Oxford Research Encyclopedia of Global Public Health. Oxford:
Oxford University Press (2021). Available online at: https://oxfordre.com/publichealth/view/10.1093/acrefore/9780190632366.001.0001/acrefore-9780190632366-e-326. doi: 10.1093/acrefore/9780190632366.013.326 -
KerrMMcCullochDOliverKMcLeanBColemanELawTet al.
Medical needs of people with intellectual disability require regular reassessment, and the provision of client- and carer-held reports. J Intell Disabil Res. (2003) 47:134–45. doi: 10.1046/j.1365-2788.2003.00453.x. PMID: -
LiaoPVajdicCTrollorJReppermundS.
Prevalence and incidence of physical health conditions in people with intellectual disability – a systematic review. PloS One. (2021) 16:e0256294. doi: 10.1371/journal.pone.0256294. PMID: -
UK Department of Health and Social Care. Valuing People: A New Strategy for Learning Disability for the 21st Century. London:
U.K. Department of Health and Social Care (2001). Available online at: https://assets.publishing.service.gov.uk/media/5a7b854740f0b62826a041b9/5086.pdf (Accessed January 21, 2026).
-
US Office of the Surgeon General (US)National Institute of Child Health and Human Development (US)Centers for Disease Control and Prevention (US). Closing the Gap: A National Blueprint to Improve the Health of Persons with Mental Retardation: Report of the Surgeon General’s Conference on Health Disparities and Mental Retardation. Washington, D.C:
US, DHHS Office of the Surgeon General (2002). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK44346/.
-
Scottish Executive Health Department. The Same as You? A Review of Services for People with Learning Disabilities. Joint Future Group of Scotland (2002). Available online at: https://www.gov.scot/publications/same-2000-2012-consultation-report/pages/7/ (Accessed January 21, 2026).
-
NSW Council for Intellectual Disability. Health and People with Intellectual Disability. Sydney, Australia:
NSW Council for Intellectual Disability (2003). Available online at: https://cid.org.au/ (Accessed January 14, 2026).
-
Ouellette-KuntzHMinnesPGarcinNMartinCLewisSMEHoldenJJA.
Addressing health disparities through promoting equity for individuals with intellectual disability. Can J Public Health. (2005) 96:S8–22. doi: 10.1007/BF03403699. PMID: -
KrahnGLHammondLTurnerA.
A cascade of disparities: Health and health care access for people with intellectual disabilities. Ment Retard Dev Disabil Res Rev. (2006) 12:70–82. doi: 10.1002/mrdd.20098. PMID: -
WHO. International Classification of Functioning, Disability and Health: ICF Vol. 299. . Geneva:
World Health Organization (2001). p. 299.
-
JanickiMPDavidsonPWHendersonCMMcCallionPTaetsJDForceLTet al.
Health characteristics and health services utilization in older adults with intellectual disability living in community residences. J Intell Disabil Res. (2002) 46:287–98. doi: 10.1046/j.1365-2788.2002.00385.x. PMID: -
LewisMALewisCELeakeBKingBHLindemannR.
The quality of health care for adults with developmental disabilities. Public Health Rep. (2002) 117:174–84. doi: 10.1016/S0033-3549(04)50124-3. PMID: -
KerrAMMcCullochDOliverKMcLeanBColemanELawTet al.
Medical needs of people with intellectual disability require regular reassessment, and the provision of client‐ and carer‐held reports. J Intell Disabil Res. (2003) 47:134–45. doi: 10.1046/j.1365-2788.2003.00453.x. PMID: -
CumellaSRansfordNLyonsJBurnhamH.
Needs for oral care among people with intellectual disability not in contact with Community Dental Services. J Intell Disabil Res. (2000) 44:45–52. doi: 10.1046/j.1365-2788.2000.00252.x. PMID: -
LinJDWuJLLeePN.
Healthcare needs of people with intellectual disability in institutions in Taiwan: Outpatient care utilization and implications. J Intell Disabil Res. (2003) 47:169–80. doi: 10.1046/j.1365-2788.2003.00454.x. PMID: -
MorganCBaxterHKerrMP.
Prevalence of epilepsy and associated health service utilization and mortality among patients with intellectual disability. Am J Ment Retard. (2003) 108:293. doi: 10.1352/0895-8017(2003)108<293:POEAAH>2.0.CO;2 -
WoodhouseJMAdlerPDuignanA.
Vision in athletes with intellectual disabilities: the need for improved eyecare. J Intell Disabil Res. (2004) 48:736–45. doi: 10.1111/j.1365-2788.2004.00595.x. PMID: -
ShavelleRStraussD.
Mortality of persons with developmental disabilities after transfer into community care: A 1996 update. Am J Ment Retard. (1999) 104:143. doi: 10.1352/0895-8017(1999)104<0143:MOPWDD>2.0.CO;2 -
McGillowaySDonnellyM.
Patterns of service use among people with learning disabilities discharged from long-stay hospital care in Northern Ireland. Ir J Psychol Med. (1999) 16:109–13. doi: 10.1017/S0790966700005401. PMID: -
NottestadJLinakerOM.
Psychiatric health needs and services before and after complete deinstitutionalization of people with intellectual disability. J Intell Disabil Res. (1999) 43:523–30. doi: 10.1046/j.1365-2788.1999.00236.x. PMID: -
LennoxTNNadkarniJMoffatPRobertsonC.
Access to services and meeting the needs of people with learning disabilities. J Learn Disabil. (2003) 7:34–50. doi: 10.1177/1469004703007001604. PMID: -
LarsonSAHewittASLakinKC.
Multiperspective analysis of workforce challenges and their effects on consumer and family quality of life. Am J Ment Retard. (2004) 109:481. doi: 10.1352/0895-8017(2004)109<481:MAOWCA>2.0.CO;2 -
DownsAWileNKrahnGTurnerA.
Wellness promotion in persons with disabilities: Physicians’ personal behaviors, attitudes, and practices. Rehabil Psychol. (2004) 49:303–8. doi: 10.1037/0090-5550.49.4.303. PMID: -
HenselERoseJKroeseBSBanks-SmithJ.
Subjective judgements of quality of life: a comparison study between people with intellectual disability and those without disability. J Intell Disabil Res. (2002) 46:95–107. doi: 10.1046/j.1365-2788.2002.00343.x. PMID: -
NerneyTViningV.
Self-determination after a decade. In: TASH ConnectionsBaltimore:
TASH (2005). p. 3–5.
-
LennoxNGGreenMDiggensJUgoniA.
Audit and comprehensive health assessment programme in the primary healthcare of adults with intellectual disability: a pilot study. J Intell Disabil Res. (2001) 45:226–32. doi: 10.1046/j.1365-2788.2001.00303.x. PMID: -
LennoxN.
ASK for it: Development of a health advocacy intervention for adults with intellectual disability and their general practitioners. Health Prom Int. (2004) 19:167–75. doi: 10.1093/heapro/dah204. PMID: -
HellerTHsiehKRimmerJH.
Attitudinal and psychosocial outcomes of a fitness and health education program on adults with Down syndrome. Am J Ment Retard. (2004) 109:175. doi: 10.1352/0895-8017(2004)109<175:AAPOOA>2.0.CO;2 -
AbdullahNHorner-JohnsonWDrumCEKrahnGLStaplesEWeisserJet al.
Healthy Lifestyles for people with disabilities. Californian J Health Prom. (2004) 2:42–54. doi: 10.32398/cjhp.v2isi.909 -
KrahnGLWalkerDKCorrea-De-AraujoR.
Persons with disabilities as an unrecognized health disparity population. Am J Public Health. (2015) 105:S198–206. doi: 10.2105/AJPH.2014.302182. PMID: -
KrahnGLFoxMH.
Health disparities of adults with intellectual disabilities: What do we know? What do we do? Res Intellect Disabil. (2014) 27:431–46. doi: 10.1111/jar.12067. PMID: -
Van Schrojenstein Lantman-de ValkHLinehanCKerrMNoonan-WalshP.
Developing health indicators for people with intellectual disabilities. The method of the POMONA project. J Intell Disabil Res. (2007) 51:427–34. doi: 10.1111/j.1365-2788.2006.00890.x. PMID: -
LinehanCWalshPNVan Schrojenstein Lantman-de ValkHMJKerrMPDawsonFon behalf of the POMONA-1 Group.
Are people with intellectual disabilities represented in European public health surveys? Res Intellect Disabil. (2009) 22:409–20. doi: 10.1111/j.1468-3148.2009.00521.x. PMID: -
PerryJLinehanCKerrMSalvador-CarullaLZeilingerEWeberGet al.
The P15 – a multinational assessment battery for collecting data on health indicators relevant to adults with intellectual disabilities. J Intell Disabil Res. (2010) 54:981–91. doi: 10.1111/j.1365-2788.2010.01322.x. PMID: -
WHO Commission on Social Determinants of HealthWorld Health Organization. Closing the gap in a generation: Health equity through action on the social determinants of health: Commission on Social Determinants of Health final report Vol. 246.
World Health Organization, Commission on Social Determinants of Health, editor. Geneva, Switzerland:
World Health Organization, Commission on Social Determinants of Health (2008). p. 246.
-
Commission of the European Communities. Solidarity in Health: Reducing Health Inequalities in the EU. Brussels:
European Commission (2009). Available online at: https://ec.europa.eu/health/ph_determinants/socio_economics/documents/com2009_en.pdf (Accessed March 10, 2026).
-
MarmotMAllenJGoldblattPBoyceTMcNeishDGradyMet al.
Fair Society, Healthy Lives: Strategic Review of Health Inequalities in England post-2010. In: Fair Society, Health Lives: The Marmot ReviewUniversity College, London (2010). Available online at: https://www.instituteofhealthequity.org/resources-reports/fair-society-healthy-lives-the-marmot-review/fair-society-healthy-lives-full-report-pdf.pdf (Accessed January 19, 2026).
-
Parliament of Australia. Evidence for the Social Determinants of Health in AUSTRALIA. Canberra:
Parliament of Australia (2010). Available online at: https://www.aph.gov.au/parliamentary_business/committees/senate/community_affairs/completed_inquiries/2010-13/socialdeterminantsofhealth/report/c02#:~:text=The%20following%20chapters%20discuss%20areas,determinants%20of%20health%20in%20Australia (Accessed January 21, 2026).
-
KohHKPiotrowskiJJKumanyikaSFieldingJE.
Healthy People: A 2020 vision for the social determinants approach. Health Educ Behav. (2011) 38:551–7. doi: 10.1177/1090198111428646. PMID: -
StankiewiczADesMeulesM.
Report summary – Rio Political declaration on social determinants of health: a snapshot of Canadian actions 2015. Health Promot Chronic Dis Prev Can. (2015) 35:113–4. doi: 10.24095/hpcdp.35.7.03. PMID: -
The Marmott Review Team. Health Inequalities in TAIWAN. Taipei:
Taiwan Health Promotion Administration, UCL Institute of Healthy Equity (2016). Available online at: https://www.instituteofhealthequity.org/resources-reports/health-inequalities-in-Taiwan (Accessed March 10, 2026).
-
MarmotMWorld Health OrganizationUCL Institute of Health Equity. Review of social determinants and the health divide in the WHO European Region: final report Vol. 188.
MarmotM, editor. Copenhagen:
World Health Organization, Regional Office for Europe (2013). p. 188.
-
Department of Developmental Disability Neuropsychiatry. Accessible mental health services for people with an intellectual disability: A guide for providers. Sydney:
Department of Developmental Disability Neuropsychiatry (2014). Available online at: https://www.3dn.unsw.edu.au/the-guide (Accessed January 28, 2026).
-
CooperSAVan Der SpeckR.
Epidemiology of mental ill health in adults with intellectual disabilities: Current Opinion in Psychiatry. Curr Opin Psychiatry. (2009) 22:431–6. doi: 10.1097/YCO.0b013e32832e2a1e. PMID: -
MelvilleCACooperSAMorrisonJSmileyEAllanLJacksonAet al.
The prevalence and incidence of mental ill-health in adults with autism and intellectual disabilities. J Autism Dev Disord. (2008) 38:1676–88. doi: 10.1007/s10803-008-0549-7. PMID: -
EmersonE.
Deprivation, ethnicity and the prevalence of intellectual and developmental disabilities. J Epidemiol Community Health. (2012) 66:218–24. doi: 10.1136/jech.2010.111773. PMID: -
EmersonEGloverG.
The ‘transition cliff’ in the administrative prevalence of intellectual disability. Tizard Learn Disabil Rev. (2012) 17:139–43. doi: 10.1108/13595471211240988. PMID: -
BaloghRBrownellMOuellette-KuntzHColantonioA.
Hospitalisation rates for ambulatory care sensitive conditions for persons with and without an intellectual disability‐a population perspective. J Intellect Disabil Res. (2010) 54:820–32. doi: 10.1111/j.1365-2788.2010.01311.x. PMID: -
ShooshtariSBrownellMDikNChateauDYuCTMillsRSLet al.
A population-based longitudinal study of depression in children with developmental disabilities in Manitoba. J Ment Health Res Intell Disabil. (2014) 7:191–207. doi: 10.1080/19315864.2013.798389. PMID: -
LeonardHGlassonEBebbingtonAHammondGCroftDPikoraTet al.
Application of population-based linked data to the study of intellectual disability and autism. In: International Review of Research in Developmental Disabilities. San Diego:
Elsevier (2013). p. 281–327. Available online at: https://linkinghub.elsevier.com/retrieve/pii/B9780124077607000086. doi: 10.1016/B978-0-12-407760-7.00008-6 -
LeonardHGlassonENassarNWhitehouseABebbingtonABourkeJet al.
Autism and intellectual disability are differentially related to sociodemographic background at birth. PloS One. (2011) 6:e17875. doi: 10.1371/journal.pone.0017875. PMID: -
HermansHEvenhuisHM.
Multimorbidity in older adults with intellectual disabilities. Res Dev Disabil. (2014) 35:776–83. doi: 10.1016/j.ridd.2014.01.022. PMID: -
McCarronMSwinburneJBurkeEMcGlincheyECarrollRMcCallionP.
Patterns of multimorbidity in an older population of persons with an intellectual disability: Results from the intellectual disability supplement to the Irish longitudinal study on aging (IDS-TILDA). Res Dev Disabil. (2013) 34:521–7. doi: 10.1016/j.ridd.2012.07.029. PMID: -
ReichardAStolzleH.
Diabetes among adults with cognitive limitations compared to individuals with no cognitive disabilities. Intell Dev Disabil. (2011) 49:141–54. doi: 10.1352/1934-9556-49.2.141. PMID: -
ReichardAStolzleHFoxMH.
Health disparities among adults with physical disabilities or cognitive limitations compared to individuals with no disabilities in the United States. Disabil Health J. (2011) 4:59–67. doi: 10.1016/j.dhjo.2010.05.003. PMID: -
TurkMALandesSDFormicaMKGossKD.
Intellectual and developmental disability and COVID-19 case-fatality trends: TriNetX analysis. Disabil Health J. (2020) 13:100942. doi: 10.1016/j.dhjo.2020.100942. PMID: -
CuypersMKoks-LeensenMCJSchalkBWMBakker-van GijsselEJLeusinkGLNaaldenbergJ.
All-cause and cause-specific mortality among people with and without intellectual disabilities during the COVID-19 pandemic in the Netherlands: A population-based cohort study. Lancet Public Health. (2023) 8:e356–63. doi: 10.1016/S2468-2667(23)00062-2. PMID: -
HendersonAFlemingMCooperSAPellJPMelvilleCMackayDFet al.
COVID-19 infection and outcomes in a population-based cohort of 17–203 adults with intellectual disabilities compared with the general population. J Epidemiol Community Health. (2022) 76:550. doi: 10.1136/jech-2021-218192. PMID: -
RawlingsGHBeailN.
Long‐COVID in people with intellectual disabilities: A call for research of a neglected area. Brit J Learn Disabil. (2023) 51:91–8. doi: 10.1111/bld.12499. PMID: -
LandesSDTurkMA.
Health equity for people with intellectual and developmental disability requires vast improvements to data collection: Lessons from the COVID-19 pandemic. Disabil Health J. (2024) 17:101539. doi: 10.1016/j.dhjo.2023.101539. PMID: -
ZaagsmaMVolkersKMSwartEAKSchippersAPVan HoveG.
The use of online support by people with intellectual disabilities living independently during COVID‐19. J Intellect Disabil Res. (2020) 64:750–6. doi: 10.1111/jir.12770. PMID: -
LunskyYJahodaANavasPCampanellaSHavercampSM.
The mental health and well‐being of adults with intellectual disability during the COVID ‐19 pandemic: A narrative review. Policy Pract Intel Disabi. (2022) 19:35–47. doi: 10.1111/jppi.12412. PMID: -
UN Department of Economic and Social Affairs. Disability and Development Report 2024: Accelerating the Realization of the Sustainable Development Goals by, for and with Persons with Disabilities. Bloomfield:
United Nations Research Institute for Social Development (2025). p. 1.
-
UN Department of Economic and Social Affairs. Un Disability and Development Report – Realizing the SDGs by, for and with Persons with Disabilities, 2018. New York:
United Nations (2019).
-
World Health Organization. Global Report on Health Equity for Persons with Disabilities. Geneva:
World Health Organization (2022). p. 1.
-
Launch of the WHO Global initiative on health equity for persons with disabilities (2025). Available online at: https://webtv.un.org/en/asset/k1b/k1bib36592#:~:text=10%20June%202025,and%20building%20the%20evidence%20base (Accessed December 22, 2025).
-
FortuneNBadlandHCliftonSEmersonERacheleJStancliffeRJet al.
The Disability and Wellbeing Monitoring Framework: Data, data gaps, and policy implications. Aust New Z J Public Health. (2020) 44:227–32. doi: 10.1111/1753-6405.12983. PMID: -
AitkenZWalmsleySM BishopGBadjiSFortuneN.
Methods used to construct disability indicators in linked administrative datasets: A systematic scoping review. Popul Health Metrics. (2025) 23:22. doi: 10.1186/s12963-025-00386-w. PMID: -
NHS England Digital. Available online at: https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/learning-disabilities-data-hub (Accessed March 10, 2026).
-
National Disability Data Asset. Available online at: https://www.ndda.gov.au/ (Accessed March 10, 2026).
-
Australian Institute of Health and Welfare. National Health Data Hub. Canberra:
Australian Government (2025). Available online at: https://www.aihw.gov.au/reports-data/nhdh (Accessed January 29, 2026).
-
Health Data Research Network Canada. Health Data Research Network CANADA [website]. Vancouver, Canada:
Health Data Research Network (2026). Available online at: https://hdrn.ca/en/ (Accessed January 19, 2026).
-
Population Data BC. Population Data BC [Website]. Vancouver, Canada:
Population Data (2026). Available online at: https://www.popdata.bc.ca/ (Accessed January 19, 2026).
-
Manitoba Centre for Health Policy. The Manitoba Population Rsearch Data Repository [Website]. Winnipeg, Canada:
Univesity of Manitoba (2026). Available online at: https://umanitoba.ca/manitoba-centre-for-health-policy/data-repository (Accessed January 21, 2026).
-
Institute for Clinical Evaluative Sciences (ICES). Institute for Clinical Evaluative Sciences (ICES) [Website]. Toronto, Canada:
Institute for Clinical Evaluative Sciences (ICES (2026). Available online at: https://www.ices.on.ca/ (Accessed January 19, 2026).
-
US DHHS Office of the Assistant Secretary for Planning and Evaluation. Dataset on Intellectual and Developmental Disabilities: Linking Data to Enhance Person-Centered Outcomes Research [news brief]. Washington, D.C:
US Department of Health and Human Services. Available online at: https://aspe.hhs.gov/dataset-intellectual-developmental-disabilities-linking-data-enhance-person-centered-outcomes (Accessed January 21, 2026).
-
SommersAChiriGRiosNHayesMPlourdeEKarimiMet al.
Operationalizing the definition of intellectual and developmental disabilities in administrative claims data for research [ASPE Issue Brief. In: Office of the Assistant Secretary for Program Evaluation. Washington (DC:
US DHHS Office of the Assistant Secretary for Program Evaluation (2025). Available online at: https://aspe.hhs.gov/reports/definition-iddd-administrative-claims-data (Accessed December 31, 2025).
-
DhopeshwarkarRJiménezFRyanSPlourdeEKarimiM.
Improving data infrastructure for person-centered outcomes research on intellectual and developmental disabilities. Am J Intell Dev Disabil. (2024) 129:231–41. doi: 10.1352/1944-7558-129.3.231. PMID: -
WeiseJCSrasuebkulPTrollorJN.
Potentially preventable hospitalisations of people with intellectual disability in New South Wales. Med J Aust. (2022) 216:161. doi: 10.5694/mja2.51390. PMID: -
ReppermundSSrasuebkulPVajdicCMPearsonSMoorinRETrollorJN.
Cohort profile: Understanding health service system needs for people with intellectual disability using linked data in New South Wales, Australia. Epidemiol Health. (2024) 7:2024054. doi: 10.4178/epih.e2024054. PMID: -
LiaoPVajdicCMReppermundSCvejicRCWatkinsTRSrasuebkulPet al.
Readmission and emergency department presentation after hospitalisation for epilepsy in people with intellectual disability: A data linkage study. PloS One. (2022) 17:e0272439. doi: 10.1371/journal.pone.0272439. PMID: -
SrasuebkulPCvejicRCHeintzeTReppermundSTrollorJN.
Public mental health service use by people with intellectual disability in New South Wales and its costs. Med J Aust. (2021) 215:325–31. doi: 10.5694/mja2.51166. PMID: -
FlorioTTrollorJ.
Mortality among a cohort of persons with an intellectual disability in New South Wales, Australia. Res Intellect Disabil. (2015) 28:383–93. doi: 10.1111/jar.12190. PMID: -
TrollorJSrasuebkulPXuHHowlettS.
Cause of death and potentially avoidable deaths in Australian adults with intellectual disability using retrospective linked data. BMJ Open. (2017) 7:e013489. doi: 10.1136/bmjopen-2016-013489. PMID: -
Australian Government Department of Health D and A. National Roadmap for Improving the Health of People with Intellectual Disability [text]. Canberra:
Australian Government Department of Health, Disability and Ageing (2025). Available online at: https://www.health.gov.au/our-work/national-roadmap-for-improving-the-health-of-people-with-intellectual-disability (Accessed January 29, 2026).
-
US HHS Administration for Community Living. I/DD Counts. Available online at: https://acl.gov/iddcounts (Accessed April 13, 2026).
-
RoseNRoseJKentS.
Staff training in intellectual disability services: a review of the literature and implications for mental health services provided to individuals with intellectual disability. Int J Dev Disabil. (2012) 58:24–39. doi: 10.1179/2047387711Y.0000000005. PMID: -
National Association for Dual Diagnosis. NADD [Website]. Kingston, New York:
NADD. Available online at: https://thenadd.org/ (Accessed January 19, 2026).
-
CostelloHBourasNDavisH.
The role of training in improving community care staff awareness of mental health problems in people with intellectual disabilities. Res Intellect Disabil. (2007) 20:228–35. doi: 10.1111/j.1468-3148.2006.00320.x. PMID: -
TrollorJN.
It’s time to address the mental health needs of people with intellectual disability. Australas Psychiatry. (2018) 26:575–6. doi: 10.1177/1039856218809770. PMID: -
CooperSABertelliMOBradleyE.
Epidemiology of psychiatric disorders in persons with intellectual disabilities. In:
BertelliMODebSMunirKHassiotisASalvador-CarullaL, editors.Textbook of Psychiatry for Intellectual Disability and Autism Spectrum Disorder.
Springer International Publishing, Cham (2022). p. 215–29. Available online at: https://link.springer.com/10.1007/978-3-319-95720-3_9. doi: 10.1007/978-3-319-95720-3_9 -
ArnoldSRHuangYSrasuebkulPCvejicRCMichalskiSCTrollorJN.
Prevalence of psychiatric conditions in people with intellectual disability: A record linkage study in New South Wales, Australia. Aust N Z J Psychiatry. (2025) 59:433–47. doi: 10.1177/00048674251324824. PMID: -
LiXTrollorJReppermundSSrasuebkulP.
Emergency department presentation and readmission after index psychiatric admission: A data linkage study. Eur Psychiatry. (2018) 48:S447–7. doi: 10.26226/morressier.5a6ef3eed462b80290b578d2 -
Disability Health Services. Available online at: https://www.qld.gov.au/health/support/people-with-disability-support-workers-and-carers/health-services (Accessed April 13, 2026).
-
Statewide Intellectual Disability Mental Health Hubs. Available online at: https://www.health.nsw.gov.au:443/mentalhealth/Pages/intellectual-disability-mental-health-hubs.aspx (Accessed April 13, 2026).
-
Victorian Dual Disability Service. Available online at: https://vdds.org.au/ (Accessed April 13, 2026).
-
England NHS. NHS England: Learning disability and autism (2024). Available online at: https://www.england.nhs.uk/learning-disabilities/ (Accessed January 29, 2026).
-
AyreJBonnerCMuscatDMCvejicEMacOMouwadDet al.
Effects of an online plain language tool on health information quality: A randomised controlled trial. In: Public and Global HealthLondon:
MedRxiv (2024). Available online at: http://medrxiv.org/lookup/doi/10.1101/2024.04.04.24305365. doi: 10.1101/2024.04.04.24305365 -
AyreJBonnerCMuscatDMDunnAGHarrisonEDalmazzoJet al.
Multiple automated health literacy assessments of written health information: Development of the SHeLL (Sydney Health Literacy Lab) Health Literacy Editor v1. JMIR Form Res. (2023) 7:e40645. doi: 10.2196/40645. PMID: -
Photosymbols.
EasyMaker. Available online at: https://www.photosymbols.com/pages/easymaker (Accessed April 13, 2026).
-
Widget Software. Available online at: https://www.widgit.com/products/widgit-online/index.htm (Accessed April 13, 2026).
-
Azure AI Immersive Reader | Microsoft Azure. Redmond, WA:
Microsoft Corporation. Available online at: https://azure.microsoft.com/en-us/products/ai-services/ai-immersive-reader (Accessed April 13, 2026).
-
Natural Reader. Available online at: https://naturalreader.net/ (Accessed April 13, 2026).
-
United Nations. Convention on the Rights of Persons with Disabilities (2006). Available online at: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html (Accessed August 5, 2026).
-
TaggartLMulhallPKellyRTripHSullivanBWallénEF.
Preventing, mitigating, and managing future pandemics for people with an intellectual and developmental disability ‐ Learnings from COVID ‐19: A scoping review. Policy Pract Intel Disabi. (2022) 19:4–34. doi: 10.1111/jppi.12408. PMID: -
WeissJAModicaPTGallantCRoudbaraniFWeaverCBoumaAet al.
Co-creating a Canadian autism mental health literacy resource: A qualitative analysis of advisory perspectives. Health Res Policy Sys. (2025) 23:140. doi: 10.1186/s12961-025-01403-y. PMID: -
O’BrienPMcConkeyRO’BrienBButlerSGarcia IriarteE.
From inclusive research to inclusive evaluation: Empowering people with intellectual disabilities to shape the services they use. Soc Sci. (2025) 15:4. doi: 10.3390/socsci15010004. PMID: -
PassmoreSRMedinaMNMackCRandolphMAusderauKK.
We don’t always know what we are missing.” Research teams’ perspectives on the recruitment of adults with intellectual and developmental disabilities in general population research. J Empirical Res Hum Res Ethics. (2025) 21:15562646251400490. doi: 10.1177/15562646251400490. PMID: -
IezzoniLI.
Ableism and structural ableism in health care workplaces. JAMA Netw Open. (2024) 7:e2430315. doi: 10.1001/jamanetworkopen.2024.30315. PMID: -
LundbergDJChenJA.
Structural ableism in public health and healthcare: A definition and conceptual framework. Lancet Reg Health – Americas. (2024) 30:100650. doi: 10.1016/j.lana.2023.100650. PMID: -
SwansonME.
Need for the Life Course Model for Spina Bifida. Pediatr Clinics North America. (2010) 57:893–901. doi: 10.1016/j.pcl.2010.08.001. PMID: -
HavercampSM.
Can You Hear Us Now? Engaging Adults with IDD in Health Research, Appendix D. In: Nisonger Center, Ohio (2023).
-
De LeeuwMJOppewalAElbersRGKnulstMWEJVan MaurikMCVan BruggenMCet al.
Healthy ageing and intellectual disability study: Summary of findings and the protocol for the 10-year follow-up study. BMJ Open. (2022) 12:e053499. doi: 10.1136/bmjopen-2021-053499. PMID: -
McCarronMHaighMDannGMcCallionP. Longitudinal dynamics in the ageing of people with an intellectual disability: Wave 5 IDS-TILDA. Dublin:
Trinity Center for Ageing and Intellectual Disability, University of Dublin (2023). Available online at: https://www.tara.tcd.ie/tara8/server/api/core/bitstreams/8e2cbce9-d149-48ca-bbed-81a1dd5e6b6f/content (Accessed March 10, 2026).
-
AkpanekpoEIButlerTSrasuebkulPTrollorJNKasinathanJGreenbergDet al.
Mental health disorders, adverse childhood experiences and accelerated reoffending among justice-involved youth in Australia: A longitudinal recurrent event analysis. Int J Law Psychiatry. (2025) 101:102099. doi: 10.1016/j.ijlp.2025.102099. PMID: -
ShooshtariSBrownellMMillsRSLDikNYuDCTChateauDet al.
Comparing health status, health trajectories and use of health and social services between children with and without developmental disabilities: A population‐based longitudinal study in Manitoba. Res Intellect Disabil. (2017) 30:584–601. doi: 10.1111/jar.12253. PMID: -
MoonenXFestenDBakker-van GijselEVervoort-SchelJ.
A Dutch perspective on two health related issues regarding children and adolescents with intellectual disabilities. IJERPH. (2022) 19:11698. doi: 10.3390/ijerph191811698. PMID: -
BurJMissenKCooperS.
The impact of intellectual disability nurse specialists in the United Kingdom and Eire Ireland: An integrative review. Nurs Open. (2021) 8:2018–24. doi: 10.1002/nop2.690. PMID: -
McCarronMSheerinFRocheLRyanAMGriffithsCKeenanPet al. Shaping the Future of Intellectual Disability Nursing in IRELAND. Dublin:
Health Services Executive, Ireland (2018). Available online at: https://www.pna.ie/images/2109181.pdf (Accessed February 10, 2026).
-
SullivanWFDiepstraHHengJAllySBradleyECassonIet al.
Primary care of adults with intellectual and developmental disabilities. Can Fam Phys. (2018) 64:254. doi: 10.1016/j.jand.2013.07.029. PMID: -
Surrey Place. Primary Care Tools. Toronto, Ontario Canada:
Surrey Place (2019). Available online at: https://ddprimarycare.surreyplace.ca/tools-2/ (Accessed January 9, 2026).
-
Association of University Centers on Disabilities (AUCD), Centers for Disease Control and Prevention. Including People with Disabilities: Public Health Workforce Competencies. Washington, D.C:
Association of University Centers on Disabilities (2016). Available online at: https://www.aucd.org/uploads/PublicHealth/updatedcompetencies-pdf-final.pdf (Accessed January 6, 2026).
-
Alliance for Disability in Health Care Education. Core Competencies on Disability for Health Care Education. Peapack, New Jersey:
Alliance for Disability in Health Care Education (2019). Available online at: http://www.adhce.org/ (Accessed January 21, 2026).
-
WHO. A Global Health Strategy for 2025–2028 advancing equity and resilience in a turbulent world: Fourteenth General Programme of Work. Geneva, Switzerland:
World Health Organization (2025). Available online at: https://iris.who.int/server/api/core/bitstreams/46cc7cac-e35e-451b-808e-1f0e4ad5f68c/content (Accessed January 19, 2026).
-
WalkerARTrollorJNFlorioTSrasuebkulP.
Predictors and outcomes of recognition of intellectual disability for adults during hospital admissions: A retrospective data linkage study in NSW, Australia. PloS One. (2022) 17:e0266051. doi: 10.1371/journal.pone.0266051. PMID: -
Government of Australia NIAA. Framework for Governance of Indigenous Data (GID) (2024). Available online at: https://www.niaa.gov.au/our-work/data-evaluation-and-research/framework-governance-indigenous-data-gid (Accessed January 31, 2026).
-
Maiam Nayri Wingara AIGI. Indigenous Data Sovereignty Communique. Canberra, ACT:
Government of Australia (2018). Available online at: https://static1.squarespace.com/static/5b3043afb40b9d20411f3512/t/63ed934fe861fa061ebb9202/1676514134724/Communique-Indigenous-Data-Sovereignty-Summit.pdf (Accessed April 13, 2026).
-
HavercampSMKrahnGLMurrayAJAkobirshoevIBellamyCDBonardiAet al.
A call to action to include disability in intersectional health equity research and policy. Lancet Reg Health – Americas. (2025) 49:101199. doi: 10.1016/j.lana.2025.101199. PMID: -
SteinPJSSteinMA.
Climate change and the right to health of people with disabilities. Lancet Global Health. (2022) 10:e24–5. doi: 10.1016/S2214-109X(21)00542-8. PMID: -
EngelmanACraigLIlesA.
Global disability justice in climate disasters: Mobilizing people with disabilities as change agents: A. Health Affairs. (2022) 41:1496–504. doi: 10.1377/hlthaff.2022.00474. PMID:
Summary
Keywords
data linkage, disability competencies, health, health disparities, intellectual disability, progress
Citation
Krahn GL and Trollor JN (2026) Improving the health of people with intellectual disability: past progress and future directions. Front. Psychiatry 17:1804423. doi: 10.3389/fpsyt.2026.1804423
Received
05 February 2026
Revised
23 March 2026
Accepted
30 March 2026
Published
21 April 2026
Volume
17 – 2026
Edited by
Helen Margaret Leonard, University of Western Australia, Australia
Reviewed by
Trine Thilsing, University of Southern Denmark, Denmark
Updates
Check for updates
Copyright
© 2026 Krahn and Trollor.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gloria L. Krahn, gloria.krahn@oregonstate.edu
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.